Electrocardiogram # 1

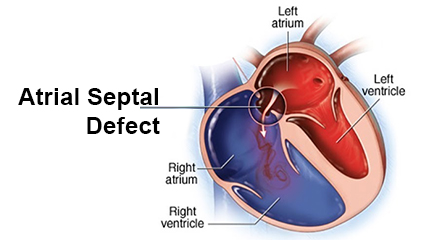
Four year old girl with a large secundum Atrial Septal Defect (ASD)
Note:
Right Axis Deviation – (QRS negative in lead 1 and positive in AVF) – a feature of Right Ventricular Hypertrophy
Right Ventricular Hypertrophy (deep S in V6 )
Right Atrial Enlargement – (tall P waves in lead 11)
RsR’ ( Incomplete RBBB in V1 )- due to right ventricular volume overload
The clinical findings associated with an atrial septal defect are subtle. There is no pressure gradient from the left to the right chamber (as with a ventricular septal defect). The right and left atrial pressures are the same. Blood therefore quietly oozes form the normally stiff left atrium to the normally more elastic right atrium filling the right heart without a murmur.
The murmur associated with an ASD is the soft physiological noise associated with increased flow of blood from the volume loaded right ventricle into the pulmonary artery. This is often missed on auscultation. The volume loaded right ventricle takes a longer time to empty .The pulmonary valve closure therefore lags behind aortic valve closure causing wide fixed splitting of the second heart sound, a feature pathognomonic of ASDs, but, is often not appreciated.
The ECG is therefore a valuable adjunct to the physical examination in differentiating children with an ASD from those with an innocent murmur.